RNA therapeutics use RNA molecules to modulate gene expression, silence disease-driving transcripts, or enable transient production of therapeutic proteins. Because RNA can be designed to engage transcripts and regulatory pathways directly, it expands the range of druggable targets beyond what small molecules and antibodies can typically address.
In practice, RNA modality choice is only half the equation. Delivery and CMC execution determine whether an RNA concept becomes a reproducible medicine with a controllable safety profile. This page maps the main therapeutic RNA types and the development constraints that matter when moving from mechanism to product.
What are RNA-based medicines?
RNA-based medicines use RNA molecules to treat disease by modulating gene expression, silencing harmful genes, or introducing therapeutic proteins. Unlike traditional drugs, which are often small molecules or antibodies that target only a small fraction (0.05%) of the human genome, RNA molecules can selectively interact with proteins, transcripts, and genes, expanding the range of druggable targets.
Why RNA types matter
RNA therapeutics is a rapidly evolving field with the potential to reshape treatment options across genetic disorders, infectious disease, and cancer. That breadth exists because “RNA therapeutics” is not one platform but a set of distinct RNA modalities, each with its own mechanism of action, potency drivers, safety liabilities, and delivery requirements.
To make the differences practical, the sections below focus on six RNA types that repeatedly appear in therapeutic development: messenger RNA (mRNA), self-amplifying RNA (saRNA), small interfering RNA (siRNA), microRNA (miRNA), circular RNA (circRNA), and transfer RNA (tRNA)-based approaches.
Types of RNAs in research
RNA research encompasses a broad range of RNA species. The main types of RNA studied include messenger RNA (mRNA), self-amplifying RNA (saRNA), small interfering RNA (siRNA), circular RNA (circRNA), microRNA (miRNA), and transfer RNA (tRNA). The following overview presents the percentage of published scientific papers focused on each RNA type within RNA research.

Types of RNAs used in RNA therapeutics
Different RNA species are used in RNA therapeutics because their mechanisms and cellular behaviors differ in ways that matter clinically. We are experts on six key RNA types (mRNA, saRNA, siRNA, circRNA, miRNA, and tRNA), based on relevance in current therapeutic development and internal capabilities to support design, synthesis, and formulation.
Messenger RNA (mRNA)
mRNA is used when the therapeutic goal is to produce a protein inside a target cell. Once delivered, the mRNA is translated into the encoded protein, which makes the platform well suited to protein replacement, vaccines, and transient expression of gene editing components.
The most practical advantages tend to be threefold.
mRNA expression is transient, which provides a built-in control mechanism and minimizes concerns about long-term genomic effects.
The platform is highly versatile because the payload is a sequence, so switching targets often means changing the coding region rather than rebuilding a new chemistry from scratch.
mRNA can be manufactured through in vitro transcription without living cells, which supports rapid, scalable production when timelines matter.
Self-amplifying RNA (saRNA)
saRNA extends the mRNA concept by including replication machinery that amplifies RNA inside the cell. In other words, saRNA can generate more protein per administered dose because the RNA template self-replicates after delivery.
This design can reduce dosage requirements and, in many contexts, extend the duration of protein expression. Those benefits are attractive in vaccines and potentially in chronic settings where durable expression improves pharmacology. However, the construct is larger and more complex than standard mRNA, which increases the burden on delivery, analytical characterization, and safety evaluation.
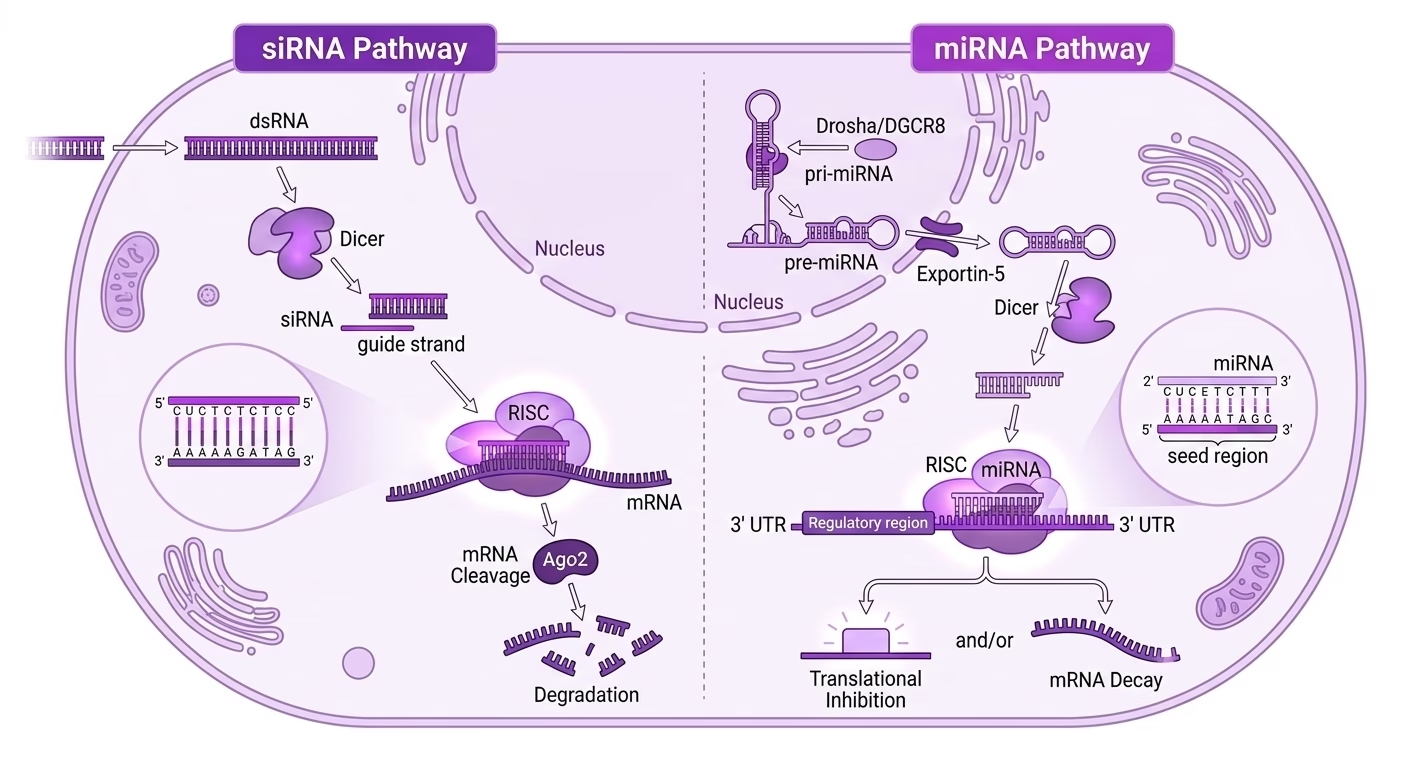
Small interfering RNA (siRNA)
siRNA is used when the goal is to silence a specific gene rather than express a new protein. These are exogenous double-stranded RNA molecules designed to bind a single target mRNA and promote its degradation, thereby reducing production of the disease-associated protein.
The value proposition is specificity and predictability. With careful design, siRNA can achieve precise transcript knockdown while limiting off-target effects. In practice, the modality’s maturity is tightly linked to delivery solutions that reliably reach the intended tissue, which is why liver-targeted siRNA programs have advanced fastest.
If the biology supports knockdown and tissue access is feasible, siRNA often offers one of the clearest mechanistic paths in RNA therapeutics.

MicroRNA (miRNA)
miRNAs are endogenous short RNAs that typically bind to the 3’ untranslated region (UTR) of target transcripts. Instead of one-to-one targeting, miRNAs often regulate networks of genes, leading to translational repression or transcript degradation across multiple pathways.
This network behavior is the main advantage and the main challenge. On one hand, miRNAs can modulate complex disease states that are not driven by a single gene. On the other hand, multi-target effects make it harder to isolate causality, manage off-target biology, and define straightforward potency readouts.
miRNA therapeutics typically require stronger translational rationale and tighter analytical strategy because the mechanism acts at the system level.
Circular RNA (circRNA)
circRNA is a naturally occurring RNA form that adopts a covalently closed loop. Because it lacks free ends, circRNA is more resistant to exonuclease degradation than linear RNA, which can translate into increased stability and potentially longer-lasting functional effects.
This stability profile is one reason circRNA is being explored for protein expression and gene regulation use cases where durability matters. Additionally, depending on sequence and structure, circRNA may evoke weaker innate immune responses than linear RNAs, although this is design-dependent and not a blanket rule.
While in 2024 circRNA was best framed as an emerging modality, the field has evolved significally by 2026 since circRNA has crossed the preclinical-to-clinical threshold. RiboX Therapeutics received the first FDA IND clearance for a circular RNA therapy and multiple companies have since followed with IND approvals from both the FDA and China’s NMPA. The field’s commercial validation came in February 2026 when Eli Lilly announced a definitive agreement to acquire Orna Therapeutics PR Newswire, whose circRNA/LNP platform is designed to generate in vivo CAR-T therapies for autoimmune disease (a use case not accessible with conventional linear mRNA).
Manufacturing scalability and immunogenicity control are now the defining development constraints as programs move from IND to first-in-human data.
Transfer RNA (tRNA)
tRNA is best known for its role in translation, delivering amino acids to ribosomes during protein synthesis. While not traditionally used as a therapeutic payload, engineered tRNA approaches are being explored in specific applications.
One active area is suppressor tRNAs designed to read through premature stop codons caused by nonsense mutations, enabling production of full-length proteins in certain genetic diseases. Another is the study of tRNA-derived fragments (tRFs or tsRNAs), which can play regulatory roles and serve as potential biomarkers. In synthetic biology, orthogonal tRNA systems enable incorporation of noncanonical amino acids into proteins, expanding protein functionality for imaging or conjugation strategies.
tRNA-based approaches are specialized and high-potential in narrow contexts, but they are not yet general-purpose platforms like mRNA or siRNA.
RNA Delivery Technologies
RNA delivery remains the dominant constraint across most RNA modalities because RNA must overcome extracellular degradation, nonspecific clearance, cellular uptake barriers, endosomal trapping, and intracellular localization requirements. For this reason, delivery is not just a formulation decision. It determines biodistribution, dose, toxicity profile, and CMC comparability risk. From a development standpoint, the delivery system effectively functions as part of the active drug.
A useful way to think about delivery options is by what they optimize: broad payload compatibility, tissue specificity, manufacturing simplicity, or local exposure.
Delivery strategies in brief:
- Lipid nanoparticles (LNPs) are broadly compatible across RNA payloads and have strong clinical precedent, particularly for systemic dosing. At the same time, they introduce multi-component complexity and can bias biodistribution toward the liver unless engineered otherwise.
- Ligand conjugates (for example GalNAc) offer highly predictable tissue targeting and simpler formulations, but they are largely tissue-limited and best suited to smaller RNAs.
- Polymeric systems provide chemical tunability and can be engineered for specific routes or tissues, although toxicity and reproducibility can become limiting factors.
- Peptide-based systems enable modular design for uptake and trafficking, often explored for local or tissue-restricted use cases, but can be variable in vivo.
- Extracellular vesicles and exosomes offer biomimetic delivery concepts, yet scalability and analytical control remain major constraints.
| Delivery approach | Strengths | Limitations | CMC Complexity |
|---|---|---|---|
|
Lipid nanoparticles (ionizable LNPs) |
Broad payload compatibility; strong clinical precedent |
Endosomal escape inefficiency; reactogenicity; complex composition |
High: particle size, lipid ratios, and process changes can alter biodistribution |
|
Ligand conjugates (GalNAc) |
Predictable liver targeting; simpler formulation |
Limited to liver; not suitable for large RNAs |
Moderate: conjugation chemistry and impurity control are critical |
|
Polymeric nanoparticles |
Chemical flexibility; customizable properties |
Toxicity risk; reproducibility challenges |
High: polymer dispersity and assembly drive CQAs |
|
Peptide systems |
Modular design; small defined components |
Variable in vivo translation; stability issues |
Moderate: peptide purity and complexation ratio are key |
|
Exosomes / EVs |
Biomimetic; targeting potential |
Heterogeneity; scalability limits |
Very high: isolation, characterization, and lot consistency |
Manufacturing and Analytical Reality
For RNA therapeutics, Chemistry, Manufacturing, and Controls (CMC) is not a downstream documentation step. CMC choices shape biological performance, safety margins, and regulatory risk, particularly when delivery systems are part of the product’s functional behavior.
Two programs with the same RNA sequence can behave differently if impurity profiles differ, particle attributes drift, or potency assays fail to detect functionally relevant changes. That is why, experienced RNA teams treat CMC and analytical strategy as part of therapeutic design.
What must be controlled, and why it matters:
- RNA identity and integrity must be confirmed at the sequence and length level, including control of truncated species. For mRNA, structural attributes such as capping and poly(A) features can directly affect translation and immunogenicity.
- Impurity profiles must be characterized and controlled because certain nucleic-acid-related impurities, including dsRNA byproducts from in vitro transcription, can trigger innate immune activation and drive tolerability signals.
- Potency assays must reflect mechanism. Translation-based modalities need expression and functional readouts, while silencing modalities require transcript knockdown and durability measurements.
- Delivery-related CQAs must be defined when the drug product includes nanoparticles or complex carriers. Particle size distribution, encapsulation efficiency, composition ratios, and shelf-life stability can shift biodistribution and safety behavior.
- Comparability strategy becomes decisive during scale-up and site changes. For complex delivery systems, comparability must show functional equivalence, not only chemical similarity.
When RNA therapies reach clinical development
RNA therapeutics require clinical strategies that differ from standard biologics because modality and delivery directly shape trial design, endpoints, and regulatory expectations.
Patient selection often relies on genetic confirmation, baseline biomarkers, or tissue accessibility, as response heterogeneity is common and enrichment is frequently necessary. Dose selection is driven by pharmacodynamic durability and expression kinetics rather than plasma exposure, leading to nontraditional redosing schedules, especially for siRNA and mRNA-based programs.
Endpoints must align with mechanism, not symptoms/biomarkers. Silencing modalities depend on transcript and protein knockdown linked to clinical benefit, while expression-based RNAs depend on the function and kinetics of the expressed protein.
Safety monitoring and bioanalysis must be tailored to modality-specific risks, with early attention to immune activation, tissue distribution, and where and when effects are measured.
Takeaway: RNA programs succeed when clinical design, endpoints, and safety strategy are built around modality-specific biology rather than borrowed from conventional biologics.
Frequently asked questions
How do I choose between mRNA and siRNA?
Choose mRNA when you need intracellular protein expression. Choose siRNA when you need transcript knockdown and reduced protein production.
Why does delivery dominate RNA feasibility?
Delivery determines which tissues receive active RNA, how much dose is required, and what safety liabilities appear first.
Are RNA therapeutics limited to the liver?
No, but liver delivery is the most mature for systemic administration. Extrahepatic delivery is possible, often via engineered carriers or local routes.
Why is CMC harder for RNA than for many small molecules?
RNA is heterogeneous by nature, and delivery systems introduce additional quality attributes that can change biological behavior.
Is circRNA clinically established?
As of 2026, circRNA has moved beyond emerging status into early clinical development, with first-in-human trials now underway and major pharma acquisition activity validating the platform.
Why do liver-targeted RNA programs advance faster than extrahepatic ones?
The liver naturally accumulates LNPs after systemic dosing due to its fenestrated vasculature, so hepatic delivery works without active targeting engineering. Every other tissue requires additional solutions (i.e., engineered carriers) each adding formulation complexity and a longer path to clinical proof of concept.
What is the biggest CMC risk during RNA-LNP scale-up?
Comparability. RNA-LNP particle size, encapsulation efficiency, and lipid composition can shift at manufacturing scale in ways that change biodistribution and efficacy without triggering standard release tests.
How does innate immune activation affect RNA therapeutic development?
Exogenous RNA can trigger pattern recognition receptors, producing cytokine responses that drive tolerability signals and suppress therapeutic effect. It is managed through chemical modifications, sequence optimization, and removal of immunostimulatory impurities like dsRNA during manufacturing.